
CASE OF DEBAKEY CLASS I AORTIC DISSECTION
Abstract
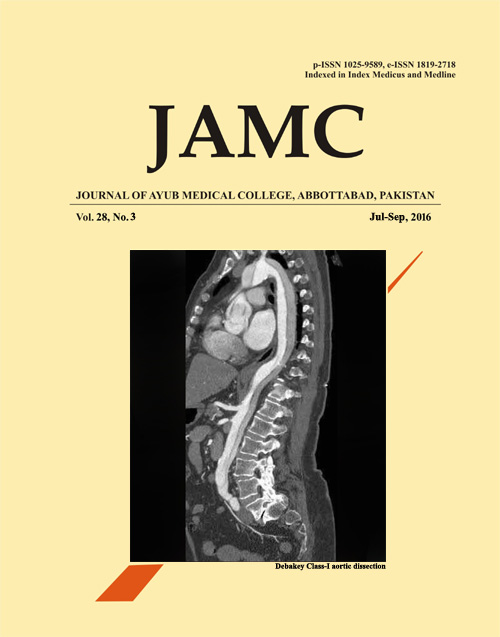
A 48 years old man presented in clinic with chest discomfort for last a week. The patient locates the pain in the middle of the chest which was episodic, with intensity of 7/10, shearing in quality and radiating to back. There were no radiating or relieving factors. The patient is a known hypertensive case for 18 years. Prior to arrival for this consult, the patient reported a loss of consciousness 5 days before after which he reported to ER with blood pressure of 155/90 mmHg and BSL of 88mg/dl. The patient was infused dextrose and was advised to maintain blood pressure. Also, the patient have not been compliant with anti-hypertensive medications. On detail history and physical exam, it was also known that patient was a smoker for past 30 years with an abnormal apex beat was noted as well. Patient also felt discomfort on deep abdominal palpation. Workups were carried, including the regular blood workup, complete metabolic profile, serum electrolyte levels with liver and renal function tests. ECG and cardiac enzymes were carries which were normal and echocardiogram was planned for the morning, when the patient had severe pain spell and was sent for the CAT scan to rule out the possibility of a mediastinal mass. On CAT scan, an aortic dissection was found. It was Debakey I/Stanford A type dissection.
Aortic dissection can be due to tear in the intima that extends forming a separate channel of blood following through it. If the disease is not addressed properly can be fatal. CAT scans can help make the diagnosis but MRI is considered the gold standard of investigation. Now aortograms, transesophageal echocardiograms are obsolete and are less popular. Ideally, the patient is kept on the drugs that can reduce the mean arterial pressure in the aorta. The best group for it is beta blockers. But if they are contraindicated due to any other comorbidity then calcium channel blockers are prescribed. This can reduce to extension of the dissection with decreasing the symptoms. Best treatment is to have a vascular intervention, either an open surgery graft or a more sophisticated endovascular aortic repair. At the dissection size of 4.5 cm, it is recommended to undergo the surgery. High blood pressure, smoking and connective tissues disorders are the contributory factors of this condition.
Downloads
Published
How to Cite
Issue
Section
License
Journal of Ayub Medical College, Abbottabad is an OPEN ACCESS JOURNAL which means that all content is FREELY available without charge to all users whether registered with the journal or not. The work published by J Ayub Med Coll Abbottabad is licensed and distributed under the creative commons License CC BY ND Attribution-NoDerivs. Material printed in this journal is OPEN to access, and are FREE for use in academic and research work with proper citation. J Ayub Med Coll Abbottabad accepts only original material for publication with the understanding that except for abstracts, no part of the data has been published or will be submitted for publication elsewhere before appearing in J Ayub Med Coll Abbottabad. The Editorial Board of J Ayub Med Coll Abbottabad makes every effort to ensure the accuracy and authenticity of material printed in J Ayub Med Coll Abbottabad. However, conclusions and statements expressed are views of the authors and do not reflect the opinion/policy of J Ayub Med Coll Abbottabad or the Editorial Board.
USERS are allowed to read, download, copy, distribute, print, search, or link to the full texts of the articles, or use them for any other lawful purpose, without asking prior permission from the publisher or the author. This is in accordance with the BOAI definition of open access.
AUTHORS retain the rights of free downloading/unlimited e-print of full text and sharing/disseminating the article without any restriction, by any means including twitter, scholarly collaboration networks such as ResearchGate, Academia.eu, and social media sites such as Twitter, LinkedIn, Google Scholar and any other professional or academic networking site.






