
GANGRENOUS GASTRITIS: UNUSUAL CAUSE OF UPPER GI BLEEDING
Abstract
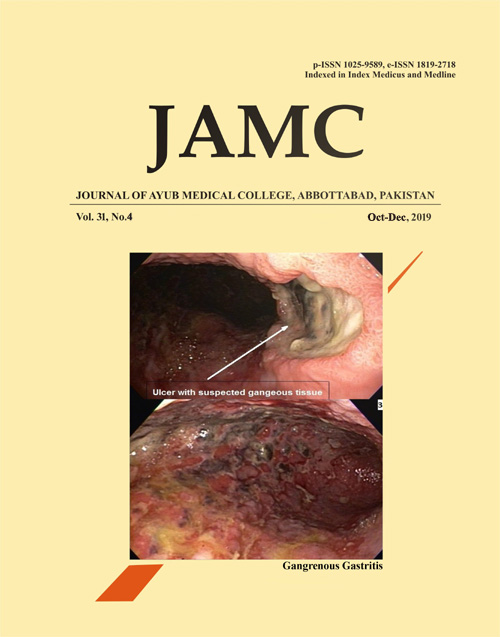
Chronic Mesenteric ischemia is an episodic hypoperfusion of small intestine due to atherosclerotic narrowing of mesenteric vessels. Typically, patients report postprandial epigastric pain. The association of abdominal pain with eating results in fear of eating and weight loss. Some patients present atypically with nausea, vomiting and/or GI bleeding likely from gut ischemia. We present here a case of 67-year-old male with history of COPD, Coronary artery disease and atrial fibrillation presented with hematemesis and black stools for one day. Patient reports no abdominal pain or weight loss. He was dizzy and nauseous. He was vitally stable and physical exam including abdominal exam was unremarkable except for the rectal exam which revealed black stools. Investigations revealed Hemoglobin of 16.1 and hematocrit of 45, WBCs of 34000 with 83% neutrophils and bicarbonate of 20. Patient underwent EGD for localizing the site of bleeding and showed stomach lumen completely filled with thrombus which prevented the accurate assessment if gastric mucosa. Repeat EGD was recommended and it revealed gangrenous appearing gastritis throughout with multiple clean ulcers which raised the suspicion of vascular compromise. CT angiography abdomen revealed complete proximal occlusion of Superior Mesenteric artery and near complete occlusion of celiac artery. He underwent successful SMA bypass from left iliac to mid SMA with PTFE graft. Symptoms of mesenteric ischemia can be non-specific and can mimic other etiologies. Clinicians should consider this diagnosis in elderly patient with risk factors of atherosclerosis as early diagnosis reduce complication associated with serious life-threatening disease.
Keywords: Gangrenous Gut, Upper GI, Bleeding, Mesenteric Ischemia, Intestinal Angina
References
ter Steege RWF, Sloterdijk HS, Geelkerken RH, Huisman AB, van der Palen J, Kolkman JJ. Splanchnic artery stenosis and abdominal complaints: clinical history is of limited value in detection of gastrointestinal ischemia. World J Surg 2012;36(4):793-9.
Pecoraro F, Rancic Z, Lachat M, Mayer D, Amann-Vesti B, Pfammatter T, et al. Chronic mesenteric ischemia: critical review and guidelines for management. Ann Vasc Surg 2013;27(1):113-22.
Oderich GS. Current concepts in the management of chronic mesenteric ischemia. Curr Treat Options Cardiovasc Med 2010;12(2):117-30.
Cognet F, Ben Salem D, Dranssart M, Cercueil JP, Weiller M, Tatou E, et al. Chronic mesenteric ischemia: imaging and percutaneous treatment. Radiographics 2002;22(4):863-80.
Nicoloff AD, Williamson WK, Moneta GL, Taylor LM, Porter JM. Duplex ultrasonography in evaluation of splanchnic artery stenosis. Surg Clin North Am 1997;77(2):339-55.
White CJ. Chronic mesenteric ischemia: diagnosis and management. Prog Cardiovasc Dis 2011;54(1):36-40.
Downloads
Published
How to Cite
Issue
Section
License
Journal of Ayub Medical College, Abbottabad is an OPEN ACCESS JOURNAL which means that all content is FREELY available without charge to all users whether registered with the journal or not. The work published by J Ayub Med Coll Abbottabad is licensed and distributed under the creative commons License CC BY ND Attribution-NoDerivs. Material printed in this journal is OPEN to access, and are FREE for use in academic and research work with proper citation. J Ayub Med Coll Abbottabad accepts only original material for publication with the understanding that except for abstracts, no part of the data has been published or will be submitted for publication elsewhere before appearing in J Ayub Med Coll Abbottabad. The Editorial Board of J Ayub Med Coll Abbottabad makes every effort to ensure the accuracy and authenticity of material printed in J Ayub Med Coll Abbottabad. However, conclusions and statements expressed are views of the authors and do not reflect the opinion/policy of J Ayub Med Coll Abbottabad or the Editorial Board.
USERS are allowed to read, download, copy, distribute, print, search, or link to the full texts of the articles, or use them for any other lawful purpose, without asking prior permission from the publisher or the author. This is in accordance with the BOAI definition of open access.
AUTHORS retain the rights of free downloading/unlimited e-print of full text and sharing/disseminating the article without any restriction, by any means including twitter, scholarly collaboration networks such as ResearchGate, Academia.eu, and social media sites such as Twitter, LinkedIn, Google Scholar and any other professional or academic networking site.






